


In spite of data suggesting that brachy boost has better outcomes for high-risk patients, it is being utilized less often and surgery is being utilized more often.
After surgery, the high-risk patient is monitored by his urologist (URO). If the URO fears a recurrence, he may
- Refer his patient to a radiation oncologist (RO) for adjuvant or salvage radiation therapy (A/SRT)
- Refer his patient to a medical oncologist if he believes the recurrence is metastatic and incurable, or
- Simply continue to monitor the patient.
The rate of utilization of A/SRT has been dwindling in spite of three major randomized clinical trials that proved that ART has better outcomes than waiting. If the patient does get to see a radiation oncologist, he may be advised to be treated soon, in conflict with the urologist advising him to wait. This puts the patient in a difficult situation.
Kishan et al. report the results of a survey among 846 ROs and 407 UROs. The researchers sought the physicians’ opinions about the conditions under which they would offer A/SRT to a high-risk, post-prostatectomy patient. For the purposes of their survey, they defined “adjuvant RT” as radiation given before PSA has become detectable, and “salvage RT” as radiation given after PSA has become detectable. “Early salvage RT” means PSA is detectable but lower than 0.2 ng/ml.
The following table shows the percentages of ROs and UROs who agreed with each survey question:
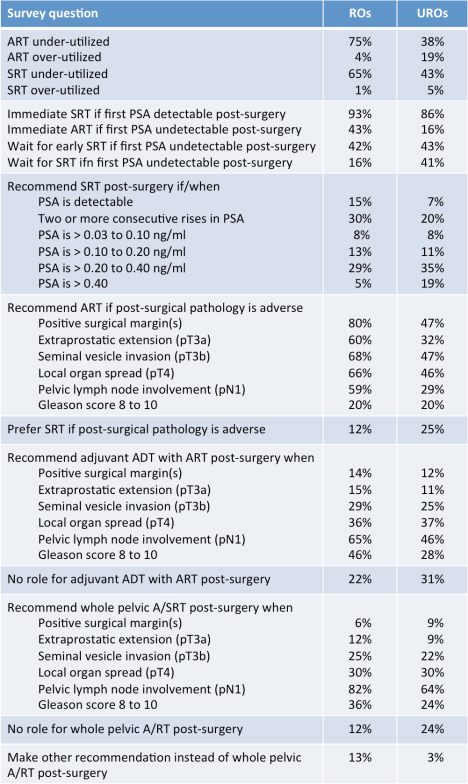
In contrast to the UROs, the ROs are more likely to believe that both ART and SRT are underutilized. UROs believe that they are used about right. ROs often see patients too late if they see them at all.
When the first PSA is detectable, both kinds of doctors would recommend SRT. When the first PSA is undetectable, 43 percent of ROs would recommend ART nonetheless, while only 16 percent of UROs would recommend ART. Most of the ROs would treat when they see two consecutive rises in PSA, or if the PSA was detectable and under 0.2. Most UROs (54 percent) would wait until PSA was over 0.2.
Over half the ROs would recommend ART to high-risk patients demonstrating any of several adverse pathological features: positive margins, stage T3/4, or positive pelvic lymph nodes. The majority of UROs would not recommend ART to high-risk patients with those adverse pathologies.
The majority of ROs (65 percent) would include adjuvant ADT if there were positive lymph nodes. UROs were less likely to recommend adjuvant ADT based on lymph node involvement and Gleason score. While most of both groups (82 percent of ROs, but only 64 percent of UROs) would have added whole pelvic radiation for patients with positive lymph nodes.
ROs, knowing that a locally advanced cancer can suddenly become metastatic, and therefore incurable, would like to give A/SRT as soon as possible. UROs, who treat patients for the combined effect of surgery and radiation on urinary and sexual function, would like to wait as long as possible. The patient is caught in the middle of this difficult decision. Some have recommended beginning neoadjuvant ADT at the lowest detectable PSA and extending that time for as long as needed to give urinary tissues maximum time to heal. Whatever the high-risk patient may eventually decide is in his best interest, he should meet with an RO immediately after surgery to hear both sides of the issue. UROs are blocking access to information that the patient needs.
Editorial note: This commentary was written by Allen Edel for The “New” Prostate Cancer InfoLink. We thank Dr. Amar Kishan for providing a full text copy of this article for Allen’s review.
Filed under: Diagnosis, Living with Prostate Cancer, Management, Risk, Treatment | Tagged: "high risk", adjuvant, post-surgery, radiation, salvage, therapy, timing |


So what I find interesting about this paper is that, although there were places where there were significant differences of opinion between the UROs and the ROs, there were other places where there was considerable similarity of opinion.
The high-risk patients remain some of the hardest patients to treat really well because some of them will respond well to first-line therapy (probably because their high-risk cancer really is organ-confined) and others just don’t respond well at all (potentially because they already have distant, micrometastatic disease).
We may not be able to resolve some of the issues here until we decide how best to conduct imaging studies prior to and immediately after first-line treatment in this set of patients. Newer and better imaging tests that are coming to market or in clinical trials may help us here.
We are probably all aware by now that traditional bone scans just don’t have the ability to identify the very high-risk patients who may be poor candidates for straightforward local treatment as first-line therapy and distinguish those men from the slightly lower high-risk patient who may indeed be curable with effective first-line therapy.
And then there is the inevitable issue of if and when the commercial interests of the RO to “do something” starts to influence the actual need to “do something” for clinical reasons (just as the commercial need of the surgeon to operate may influence his/her recommendation for surgery in the first place).
While I agree with Allen that it would be a good idea for any high-risk patient to consult with an RO immediately after he has the pathology report from his surgery, there is also an argument that the same patient would be wise to consult with an RO before he has the surgery so that he has a clear idea of what he might need to address (and how) even if he has already decided to have surgery as a first-line treatment.
Patient psychology is also a factor here. Shortly after my surgery, I consulted a RO, who recommended ART based on adverse surgical pathology. I remember how depressing it was to hear so soon after surgery that I needed yet another treatment. But when I talked to my surgeon, he strongly disagreed, saying I should wait for PSA to rise before getting RT. His opinion instantly lifted my spirits! I still agonized over the decision, but the psychological boost I got from my surgeon’s opinion led me — perhaps wrongly — to go with that recommendation.
Good point about seeing an RO even before the prostatectomy. The high-risk patient should have a clear understanding of adjuvant and salvage RT, the probability of its success and its toxicity.
I also like the idea of advanced PET scans for the high-risk patient. While most PET scans are approved for recurrent prostate cancer, I think there is opportunity for its use with high-risk prostate cancer. I know that UCLA is offering the Ga-68-PSMA scan for high-risk patients now for $2,650 (their cost). But it raises an interesting question: if distant metastases are discovered by the scan, will insurance/Medicare still pay for radical treatment of the prostate (de-bulking)? Perhaps the patient is better off not knowing until afterwards (assuming that there is a survival benefit to de-bulking).
Allen:
Based on their 20+ years of experience, I suspect the people at the Mayo Clinic would tell you that there is a survival benefit associated with debulking (in their opinion), but I can see no way to do a randomized trial because I suspect it would be unethical to randomize patients to either arm of such a trial.
M. D. Anderson Cancer Center has such a trial running now. It is ethical because the benefit, if there is one, remains unproven. Patients are randomized to debulking or standard of care, and get to choose between surgery or radiation. The University of Texas Southwestern has a registry. Outside of a clinical trial or a registry, insurance can be a problem. I’ve heard from patients who have trouble convincing insurance to pay for it because they deem it experimental.
I am acutely aware of the MDA Phase II trial on cytoreductive surgery in metastatic men and the next Phase III version under consideration. I do believe there is a benefit to the procedure but how much so has never been determined. I believe the established primary and secondary endpoints are very interesting but I cannot as yet comment on them. Last fall at SWOG, we held a special symposium on it hosted by Dr. Chapin (the PI in the link in Allen’s response) and the MDA team was received very well. In my opinion, patients diagnosed with metastatic disease want this trial. That takes the ethics out of discussion. With three “safe” arms, randomization won’t be difficult. MDA had no issues recruiting the Phase II trial. I have no reason to believe that a Phase III multi-center trial would be any different.
Anecdotally, over the past 18 months or so, I am seeing more frequent use of debulking metastatic men either with surgery or radiation. I even know of one instance where Kaiser used SBRT to debulk.
I have to wonder whether administering ADT impacts the answers to the questions by both rad oncs and surgeons — and the timing of treatment and referrals.